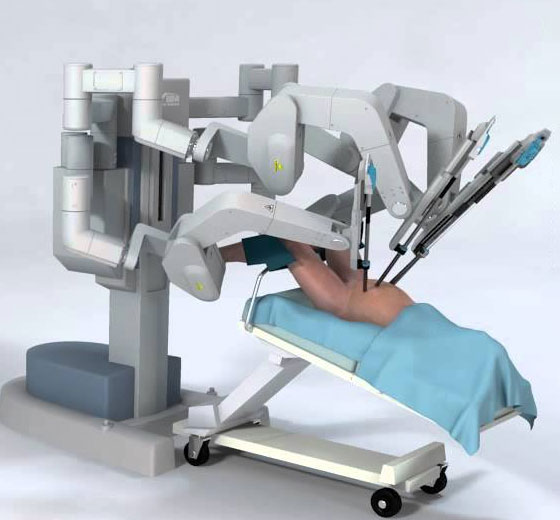
Robotic Radical Prostatectomy is a minimally invasive robotic surgery in Kerala used for Prostate Cancer Treatment . During the procedure, a surgeon uses a robotic system to remove the entire prostate gland and surrounding tissue.
Robotic radical nephrectomy is a robotic surgical procedure that involves the removal of a kidney, along with the surrounding tissues and lymph nodes, using a robotic system.
Robotic Partial Nephrectomy is a minimally invasive robotic surgery used to remove a portion of the kidney affected by a tumor or other abnormal growth.
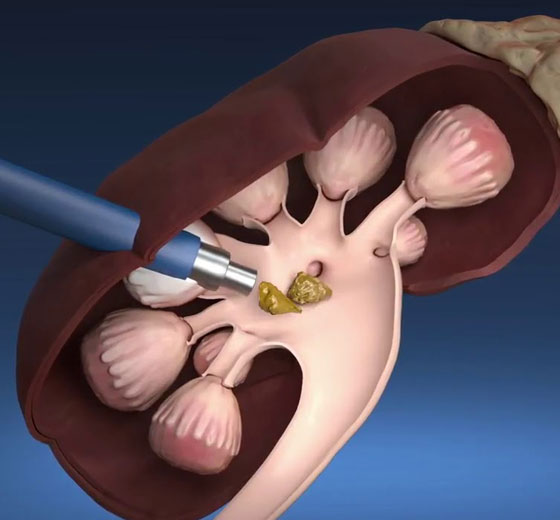
Retrograde Intra Renal Surgery (RIRS) is a minimally invasive surgical procedure used to treat kidney stones and other conditions affecting the urinary tract.
Urethroplasty is a surgical procedure used to treat urethral strictures, which are narrowings or blockages in the urethra, the tube that carries urine from the bladder out of the body.
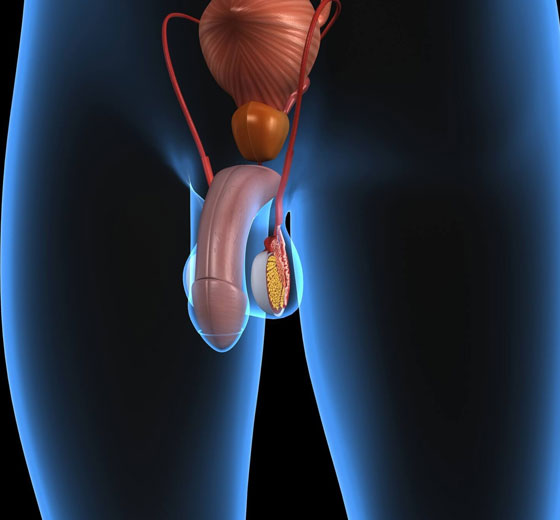
Penile Prosthesis Procedure is a surgical procedure used to treat erectile dysfunction (ED) in men who have not responded to other treatments such as medication or vacuum erection devices.
Microscopic sub-inguinal varicocelectomy is a surgical procedure that is used to treat varicoceles, which are enlarged veins in the scrotum that can cause pain, discomfort, and infertility.
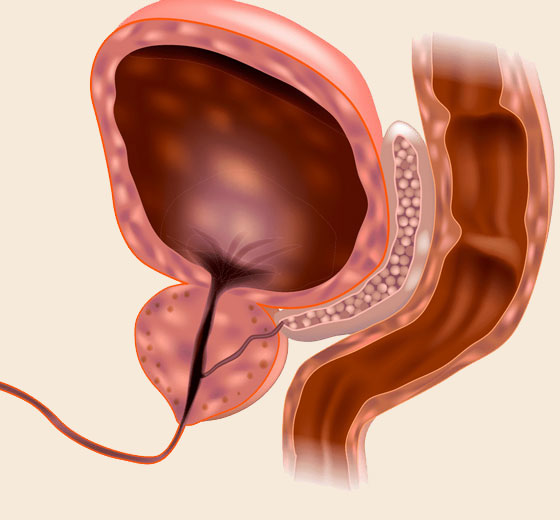
The UroLift system is a simple procedure that uses small implants to lift and hold enlarged prostate tissue, allowing for unobstructed urine flow. It does not involve cutting, heating, or removing any prostate tissue.
The procedure is generally carried out by a robot, which consists of small tools attached to a robotic arm that is controlled by a computer. One of the most widely used robotic systems in the world is the “Da Vinci system”.